

Guidelines in Practice Webinar Series
Please join us for our Guidelines In Practice webinar series!
November 3, 2025 • JASE
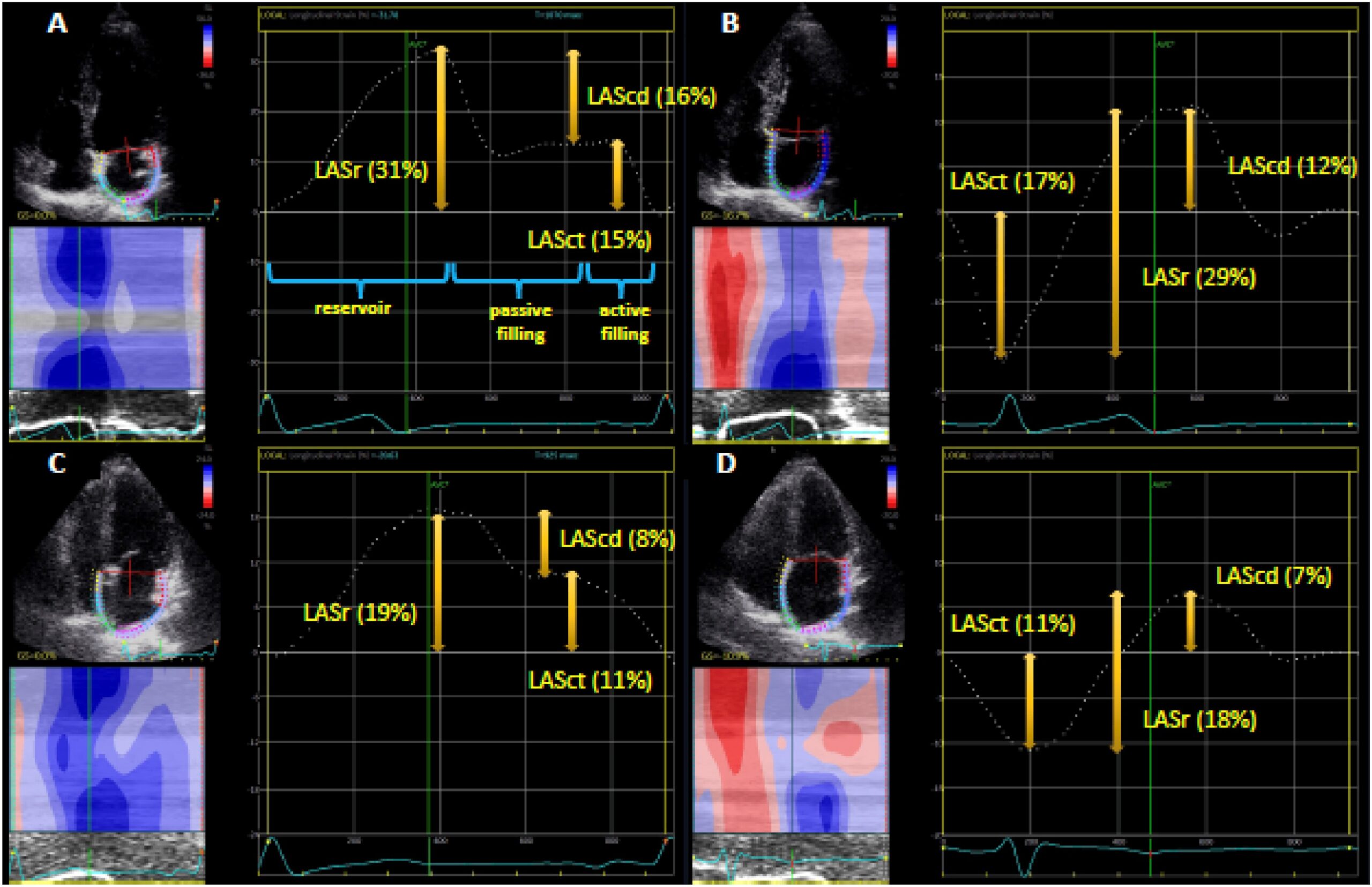
Clinical Applications of Strain Echocardiography
Clinical Applications of Strain Echocardiography: A Clinical Consensus Statement From ASE Developed in Collaboration With the EACVI
November 2, 2023 • JASE
COVID-19 Statement Update
ASE COVID-19 Statement Update: Lessons Learned and Preparation for Future Pandemics
January 27, 2021 • JASE
Adapting Pediatric, Fetal and CHD Services COVID-19
ASE Statement on Adapting Pediatric, Fetal, and Congenital Heart Disease Echocardiographic Services to the Evolving COVID-19 Pandemic
May 19, 2020 • JASE
Reintroduction of Echo During COVID-19
ASE Statement on the Reintroduction of Echocardiography Services During the COVID-19 Pandemic
April 7, 2020 • JASE
ASE Statement on COVID-19
ASE Statement on Protection of Patients and Echocardiography Service Providers During the 2019 Novel Coronavirus Outbreak: Endorsed by the American College of Cardiology
Guideline News
ASE News
Press Release
ASE Releases New Guidelines to Standardize Adult Echo Reporting
September 25, 2025
Press Release